effect of normobaric hypoxia on auditory sensitivity
Dougal B Watson MBBS,
DAvMed
Russell L Martin PhD
Sean E Smith BA(Hons)
Ken I McAnally PhD
and David L Emonson MSc MBBS
Abstract
Previous psychophysical studies of hypoxia's effects on auditory sensitivity
have provided mixed results but the weight of evidence supports the conclusion
that sensitivity is unaffected by hypoxia. This conclusion is discrepant with
that drawn from physiological studies in which hypoxia has been found to affect
auditory-evoked response (AER) latency. One possible explanation of this
discrepancy concerns the relatively low maximum frequency (8 kHz) for which
hypoxia's effects were assessed in the psychophysical studies. We have extended
the range of frequencies over which hypoxia's effects have been examined to
include frequencies up to 16 kHz. Thresholds for 1, 8, 10, 12, 14 and 16 kHz
tones were measured at levels of hypoxia equivalent to altitudes of 0, 1200,
2400 and 3700 m. Our results indicate that sensitivity for frequencies up to 16
kHz is unaffected by hypoxia. We suggest that AER latency does not always
provide a valid measure of auditory sensitivity.
Key Words: hypoxia, auditory sensitivity, auditory threshold, hearing
threshold
Introduction
The effect of hypoxia on auditory sensitivity has been examined in a number
of studies. In one of the earliest, Gellhorn and Spiesman observed that hypoxia
equivalent to that experienced on exposure to an altitude of 6100 m and induced
by breathing an appropriate gas mixture resulted in a significant decrease in
auditory sensitivity. Other studies in which hypoxia was found to reduce
sensitivity include those by McFarland, Klein and Klein et al.. In each of these
studies, hypoxia was observed to reduce sensitivity to a subset of the 5-8 pure
tone frequencies that were tested but either enhance or leave unaltered
sensitivity to the remainder. Other studies, however, suggest that auditory
sensitivity is unaffected by hypoxia. This conclusion is supported by the early
studies of Lewis (18) and Bagby, who found that hypoxia induced by exposure to
simulated altitudes high enough to result in "general functional impairment" and
loss of consciousness had no effect on absolute thresholds for air or bone
conducted sounds, and more recent studies by Curry and Boys and Burkett and
Perrin. The study by Burkett and Perrin is the most comprehensive carried out to
date and compared thresholds for six air conducted pure tones ranging in
frequency from 250 to 8000 Hz measured at ground level and simulated altitudes
of 4600 and 6100 m. Thresholds were found to be unaffected by hypoxia for all
frequencies tested. The weight of evidence from the above studies suggests that
auditory sensitivity is unaffected by hypoxia.
Hypoxia’s effects on the auditory system have also been examined using
auditory-evoked response (AER) techniques. Deecke et al., Carlile et al.,
Carlile and Paterson, Fowler and Lindeis, Lucertini et al. and Wesensten et al.
found that the latencies of various waves in human AERs increased significantly
with increasing hypoxia level. Some of these authors argued that wave
latency provides an objective measure of auditory sensitivity and interpreted
the latency increases they observed as evidence of a hypoxia-induced reduction
in sensitivity. Using stimulus-level versus wave-latency functions measured for
each of their subjects at sea level, Carlile and Paterson calculated that the
latency increases observed in their study correspond to an average reduction in
sensitivity of about 9 dB. In contrast, Mosko et al., Sohmer et al., Urbani and
Lucertini and Bouchet et al. found that AER wave latencies were unaffected by
hypoxia. This discrepancy may be accounted for in part by inter-study
differences in the duration of exposure to hypoxia prior to AER recording. The
studies by Mosko et al., Sohmer et al. and Bouchet et al. involved
particularly brief (1-2 minute) or long (24 and 72 hour) exposures that have
been found by others to be outside the range associated with latency increases.
Urbani and Lucertini, however, used exposures that were similar in duration to
those used by Carlile et al. , Lucertini et al. and Wesensten et al. and
it is unclear why they did not observe the latency increases described by these
other authors.
On the assumption that AER wave latency does provide an objective measure of
auditory sensitivity, the above studies in which hypoxia was found to induce
latency increases seem inconsistent with those in which hypoxia was observed to
have no effect on psychophysical thresholds. This discrepancy cannot be
explained with reference to the way in which hypoxia was induced, as both groups
of studies included instances in which normobaric and hypobaric hypoxia were
involved. It can, however, be partially explained with reference to the length
of time subjects were exposed to hypoxia prior to the assessment of its effects.
In the study by Burkett and Perrin referred to above, subjects were exposed to
each simulated altitude for only five minutes before threshold measurement
began. Carlile et al. found that latency increases do not develop until subjects
have experienced hypoxia for at least 20 minutes and suggested that the shorter
pre-measurement exposure period employed by Burkett and Perrin could
explain their failure to observe an effect. The length of time subjects in the
studies by Lewis and Bagby were exposed to hypoxia prior to threshold
measurement is unclear but as each session in the study by Bagby was completed
within 30 minutes, it is unlikely that in that case it was greater than a few
minutes. In the study by Curry and Boys, however, thresholds were measured
following 30 minute's exposure to hypoxia, so the fact that they did not observe
an effect of hypoxia cannot be explained in this way.
Another possible explanation of this discrepancy concerns the range of
frequencies tested in the above psychophysical studies. In keeping with most
audiometric studies, these psychophysical studies only considered frequencies up
to 8 kHz. Human hearing, however, extends to considerably higher frequencies and
it is possible that hypoxia has effects on thresholds for frequencies above 8
kHz. The cochlea’s sensitivity to high frequency sound in particular is
dependent on the integrity of active cochlear processes that are likely to be
especially vulnerable to hypoxia. As the majority of the above studies in which
hypoxia-induced wave latency increases were observed involved stimuli with
sudden onsets and AERs to such stimuli are thought to be dominated by responses
to high frequency components a hypoxia-induced reduction in sensitivity to high
frequencies may have underlied the latency increases observed.
In this study, therefore, we extended the frequency range over which
hypoxia’s effect on auditory thresholds has been examined to cover frequencies
up to 16 kHz. Thresholds for six frequencies ranging from 1 to 16 kHz were
measured following at least 15 minute's exposure to simulated altitudes of 0,
1200, 2400 and 3700 m. As an additional 40-50 minutes were required to complete
all measurements at each simulated altitude, the duration of exposure to hypoxia
at the time of threshold measurement for subjects in this study must have fallen
within the range associated with AER wave latency increases. Ideally, the range
of simulated altitudes would have extended above 3700 m but that possibility was
precluded on consideration of ethical issues.
Methods
Subjects
Four healthy, right-handed volunteers, one female and three male, ranging in
age from 24 to 26 years participated in this study. Informed consent was
obtained from each. The hearing of each subject was checked prior to testing by
measuring their absolute thresholds for 1, 2, 4, 8, 10, 12, 14 and 16 kHz tones
using the psychophysical procedures described below. For all subjects no
threshold exceeded the relevant age-specific norm by more than two
standard deviations.
Design
Thresholds were measured for six frequencies (1, 8, 10, 12, 14 and 16 kHz) at
each of four simulated altitudes (0, 1200, 2400 and 3700 m). Each subject
participated in four experimental sessions during each of which a different
altitude was tested. The order in which altitudes were tested was
counterbalanced across the four subjects using a Latin square.
Induction of hypoxia
Hypoxia was induced by having subjects breathe an appropriate gas mixture
through an aviator’s oxygen mask. Mixtures having oxygen concentrations of 21.0,
18.1, 15.6 and 13.3 % were used to simulate altitudes of 0, 1200, 2400 and 3700
m, respectively. All were blended from bottled air, oxygen and nitrogen no more
than 30 minutes before the session in which they were used and stored in 100 l
Douglas bags until needed. Testing in each session did not begin until the
subject had breathed the relevant gas mixture for at least 15 minutes and their
blood oxygen saturation level, which was monitored throughout via non-invasive
pulse oximetry, had stabilised at an altitude-appropriate level. The saturation
levels at which individual subjects stabilised as a function of altitude are
shown in Table 1. An interval of at least one hour separated all pairs of
consecutive sessions. No subject experienced hypoxia for more than two sessions
on any day.
|
Altitude (m)
|
Subject 1 |
Subject 2 |
Subject 3 |
Subject 4 |
|
0
|
99 |
97 |
97 |
98 |
|
1,200
|
96 |
95 |
96 |
95 |
|
2,400
|
95 |
92 |
84 |
93 |
|
3,700
|
89 |
86 |
85 |
89 |
|
Table 1. Blood oxygen
saturation levels (%) for individual subjects as a function of altitude.
|
Threshold measurement
Thresholds were measured using a two-interval forced-choice task combined
with the two-down one-up adaptive procedure described by Levitt. Each
measurement involved the presentation of about 40 trials during each of which
the subject's task was to determine which of two intervals coincided with the
presentation of a brief auditory signal. The occurrence of each interval was
signalled by the illumination of a light-emitting diode placed directly in front
of the subject. Each interval was 200 ms in duration and the two were separated
by 600 ms. On the initial trial the signal level was set well above the
subject’s expected threshold and on subsequent trials it was adjusted following
a two-down one-up rule in steps of 5 dB until the third reversal, then 2 dB
until the eleventh. Threshold was defined as the average of the signal levels
associated with the last eight reversals.
All thresholds were measured with the subject seated at the centre of a 3 x 3
m, sound-attenuated chamber, the background noise level within which was less
than 10 dB SPL in all 1/3-octave bands with centre frequencies from 0.5 to 16.0
kHz. Two-hundred millisecond pure-tone pulses, incorporating 10 ms rise and fall
times, were generated by a PC-controlled digital signal processing system
(Tucker-Davis Technologies System II) and presented to the subject via
headphones (Sennheiser ). The at-eardrum sound levels produced by this system
were measured by a sound level meter (Brüel and Kjær) with a 1-inch microphone (Brüel
and Kjær) in an artificial ear (Brüel and Kjær ). A button box interfaced with
the controlling PC provided the subject with a means of initiating each trial
and indicating the interval during which he/she thought the signal had been
presented.
When screening subjects prior to testing, their thresholds were measured
first for the left ear and then for the right. For each ear, thresholds were
measured twice for each frequency, following an ascending then a descending
order, and the averages were compared with the relevant norms. During testing,
however, thresholds were measured for one ear only. This ear was the left for
two of the subjects and the right for the others. Thresholds were measured three
times for each frequency and the median was taken as a representative value. In
our experience the median has proven to be a more reliable measure than the mean
with respect to threshold measurements of this type. Each experimental session
contained three blocks of threshold measurements, in each of which one
measurement was made at each frequency in a random order. About 45 minutes were
required to make all 18 measurements.
All procedures followed in this study were approved by the Australian Defence
Force Medical Ethics Committee.
Results
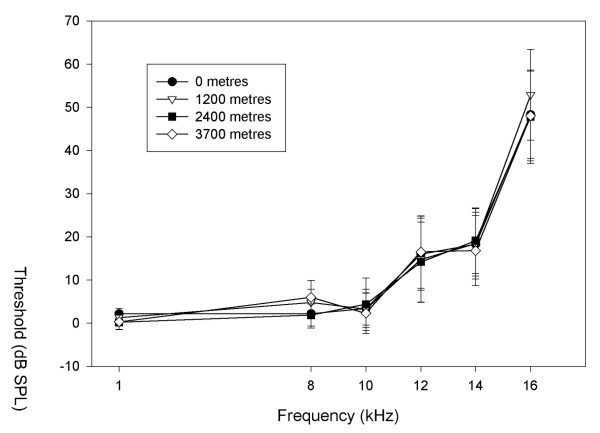
Thresholds averaged across all four subjects are plotted as a function of
frequency and simulated altitude in Figure 1. At an altitude of 0 m (solid
circles in the figure) thresholds increased with increasing frequency in a
pattern generally consistent with that for published norms. Threshold values,
however, were somewhat lower than the relevant norms for all frequencies other
than 1 kHz. This discrepancy may reflect the use of different psychophysical
and/or calibration procedures in our and the norm-defining studies. At other
altitudes thresholds varied with frequency in a similar manner and for any given
frequency, data points for all four altitudes tended to overlap. There was no
apparent effect of altitude on sensitivity at any frequency. This was confirmed
by an analysis of variance, incorporating a Greenhouse-Geisser correction, which
revealed a significant effect of frequency (F(1.4,4.19)=14.51, p=.015) but no
effect of altitude (F(1.56,4.67)=.56, p=.563) or frequency-by-altitude
interaction (F(2.29,6.87)=1.97, p=.21). Estimates of omega-squared for the
frequency and altitude treatments were calculated to be .287 and -.014,
respectively. The negative value for altitude suggests that this treatment has a
negligible effect (14). A power analysis following the procedures outlined by
Keppel revealed the presence of sufficient power (³
.8) to reliably detect an altitude effect of 4-5 dB.
|
Figure 1. |
|
|
|
Thresholds averaged across all subjects as
a function of frequency and simulated altitude.
|
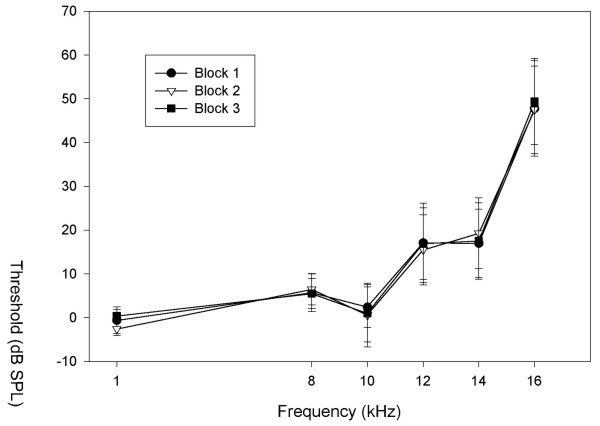
As threshold measurements at each altitude were blocked, the three threshold
measurements at each frequency were made following different durations of
exposure to hypoxia. The extent to which auditory sensitivity varied with
duration of exposure can therefore be determined by comparing thresholds across
blocks. In Figure 2 this comparison is made for the 3700 m altitude level where
an altitude effect was most likely to have been apparent. It can be seen that
for any given frequency, thresholds for the three blocks were practically
identical. This was confirmed by an analysis of variance, incorporating a
Greenhouse-Geisser correction, which revealed a significant effect of frequency
(F(1.51,4.53)=13.28, p=.014) but no effect of block (F(1.02,3.07)=.15, p=.73) or
frequency-by-block interaction (F(2.42,7.26)=.41, p=.717). This result indicates
that sensitivity was stable throughout the 40-50 minute period during which
these thresholds were measured and precludes the possibility that an altitude
effect present for only a portion of that period was obscured in the preceding
analysis in which thresholds from different blocks were combined.
|
Figure 2.
|
|
|
|
Effect of block on average thresholds at
3700 m.
|
Discussion
The results of this study indicate that auditory sensitivity for frequencies
up to 16 kHz is unaffected by hypoxia induced by exposure to simulated altitudes
as high as 3700 m.
As discussed above, studies that have used AER techniques to examine
hypoxia's effects on the auditory system have found that the latencies of
various waves in human AERs increase significantly with increasing hypoxia
level. These latency increases have been interpreted as evidence of decreased
auditory sensitivity, as at constant levels of hypoxia they are associated with
reduced stimulus levels. Carlile et al. have suggested that the discrepancy
between these studies and those in which hypoxia was observed to have no effect
on auditory thresholds resulted from differences in pre-measurement
exposure to hypoxia. Whereas subjects in Burkett and Perrin's study were exposed
to each simulated altitude for only 5 minutes before threshold measurement
began, Carlile et al. found that latency increases do not develop until subjects
have experienced hypoxia for at least 20 minutes. In the study described here,
however, threshold measurement did not begin until subjects had been exposed to
each simulated altitude for at least 15 minutes and required an additional 40-50
minutes to complete. The duration of exposure to hypoxia prior to threshold
measurement, therefore, coincided with the range associated with AER latency
increases and differences with respect to that variable cannot account for
differences between the findings of our and the AER studies.
An alternative explanation of the discrepancy between previous psychophysical
and AER studies is that latency increases observed in the AER studies resulted
from a hypoxia-induced reduction in sensitivity to frequencies greater than the
8 kHz maximum tested in the psychophysical studies. That possibility prompted us
to extend the range of frequencies over which hypoxia's effects on sensitivity
have been examined to cover frequencies up to 16 kHz. The fact that thresholds
for all frequencies tested in this study, which included five in the range from
8 to 16 kHz, were found to be unaffected by hypoxia, indicates that this
explanation also is untenable.
A more likely explanation of the discrepancy between these studies is that
AER wave latency does not always provide a valid measure of auditory
sensitivity. As noted above, authors who have interpreted wave latency increases
as evidence of decreased auditory sensitivity have done so on the basis of the
well-established association between wave latency and stimulus level. The
existence of this association, however, does not justify the use of wave latency
as a sensitivity measure. A variable such as level of hypoxia could affect wave
latency via a mechanism that has no effect on auditory sensitivity. A prime
candidate for such a mechanism, considered in two of the above reports, involves
the time required to transmit information from the auditory receptor to the site
of wave generation. A disassociation between AER wave latency and auditory
sensitivity with respect to hypoxia 's effects is suggested by the fact that
hypoxia exposures capable of inducing latency increases have been found in
several studies to have no effect on wave amplitude.
The absence of a hypoxia effect as demonstrated in this study is encouraging
with respect to the continued development and use of auditory displays in
environments such as aircraft cockpits where operators are in many cases
routinely exposed to low levels of hypoxia and at risk of exposure to much
higher levels. As hypoxia levels normally experienced by operators of modern
aircraft are lower than the maximum in this study, our results indicate that no
hypoxia-induced loss of auditory sensitivity will normally be experienced in
that environment and the auditory modality should provide an uncompromised
channel for information transfer. It is possible, however, that this will not
remain the case where operators are exposed to higher levels. Severe levels of
hypoxia (blood oxygen saturation levels of less than 65%) in non-human subjects
have been found to induce significant reductions in cochlear sensitivity, as
measured by indices such as evoked-otoacoustic-emission amplitude (24) and AER
threshold, and it seems reasonable to expect that audition will eventually be
compromised as hypoxia is increased. Arguing against this, however, is the study
by Bagby, in which exposure to hypoxia levels high enough to result in loss of
consciousness was found to have no effect on auditory thresholds.
|